
Sun S et al. eLife Sciences 2013;2:e00435
Viruses are living creatures, the smallest of all, even though they do not fulfil the definition we are familiar with. They are not even an unicellular living thing. They are not "the basic unit of life", though they are definitely alive.
They have a short segment of DNA or RNA with only a few genes with the genetic code to synthesise a few types of small proteins that are capable to self-assembling (jigsaw-puzzle-like matching and attracted by electric charges like magnets) and make another copies of itself. In order to do so the virus need to get in contact with the surface of a cell, specifically a tree-like molecular structure called proteo-glycan that pops out from the outer side of cellular membranes. To get attached to these "reseptors" viruses have 'structural proteins' in their outer layer that make perfect match with the specific proteo-glycan of an specific kind of cell from a specific kind (or few kinds) of living things.
Chikungunya virus (CHIKV) has external "E proteins" that trigger an immune respond from the host. The anti-bodies from an infected individual can be obtained by "purification" of its blood plasma and used to protect another person that has just being infected but has a less strong immunologic respond against the virus.
"Many studies have analysed the interaction of antibodies with alphaviruses (Meyer and Johnston, 1993; Griffin et al., 2001; Hunt et al., 2010). Most neutralizing antibodies bind to E2, as this glycoprotein is more exposed on the viral surface than E1."That is much easier to do than synthesising an antigen, that could be one of its "E proteins", and trial it in animals expecting that this was the antigen that conferred immunity against the virus. We have to consider also the likely possibility of mutations on "E proteins" that would make such kind of vaccine useless.
Another option for a vaccine are virus-like particles (VLP)
"Expression of the CHIKV structural C-E3-E2-6K-E1 polyprotein gives rise to virus-like particles (VLPs) that have been used to immunize and protect non-human primates against CHIKV infection (Akahata et al., 2010). Non-human primates immunized with these VLPs developed high-titer neutralizing antibodies that protected against viremia after high-dose challenges."Three-dimensional imagining studies have proved defect in the way that some "E proteins" in the CHIKV-VLP are exposed to the white blood cells reducing the chances of an appropriated immune respond.
To reach its first aim (the cellular surface) viruses relay on different means of transport because they do not have any locomotion structures such as cilia, flagella, wings or legs. So, probably, millions of years of evolution and coexistence with the rest of us (protozoans, unicellular and multicellular eukaryotes including complex plants and animals) made them so efficient in finding their way from one species to another through little droplets in a sneezing spray, on a fly legs or a mosquito's saliva.
Once attached to the target the virus finds the way to "inject" its genetic material and a few non-structural proteins inside the cell's cytoplasm. Then they (DNA/RNA plus proteins) can be transported to the host nucleus where its genetic material is integrated to the latter. The host cell will start synthesising its own proteins as usual and additionally the proteins and DNA/RNA that the virus needs to replicate itself. The other option, as in the case of CHIKV, the RNA strip replicates in the cytoplasm and the copies start synthesicing the estructural and no-structural proteins that will self-ensemble to produce as many copies as possible with the host material.
http://elifesciences.org/content/2/e00435

Chikungunya virus, is an alphavirus that knows how to infect mosquitoes, invertebrates and vertebrates. Alphavirus have no good mechanism of genetic damage repair producing many mutants in every host. The huge number of mutation can improve their "fitness" to infect, replicate and avoid the host's immune system.
http://jvi.asm.org/content/85/2/1025.long
In 2005 - 2006 there was an epidemic in Africa and Asia that reached the French territory of 'La Reunion' Island calling the attention of the developed world. During this epidemic the CHIKV infected millions of people giving it the opportunity to mutate and evolve stronger and more virulent. This epidemic was facilitated by the great population of humans in urban areas coexisting with the vector: Aedes aegipty and Aedes albopictus. For the same reason we are having a chikungunya fever epidemic spread in the Americas and Caribbean Islands.
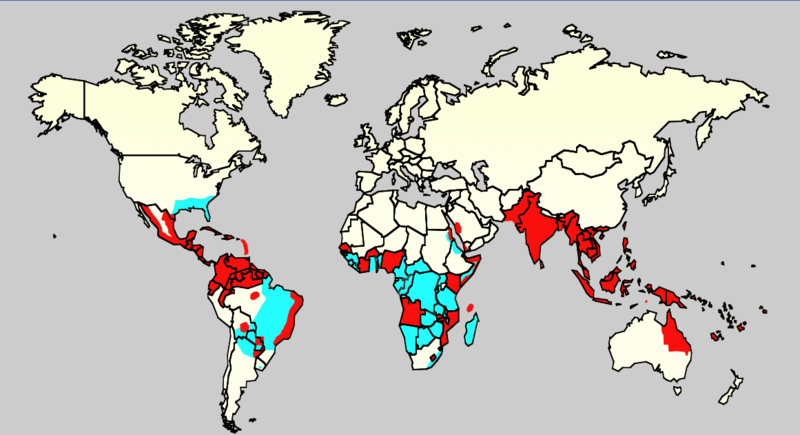
Distribution in 2006 of Aedes aegypti (blue) and epidemic dengue (red)
It caught my attention how a Panamerican Health Organization (PAHO) and the World Health Organization (WHO) programme of eradication of these vectors could have change the course and dimensions of the Chikungunya/Dengue epidemic in the Americas if it had continued and extended.
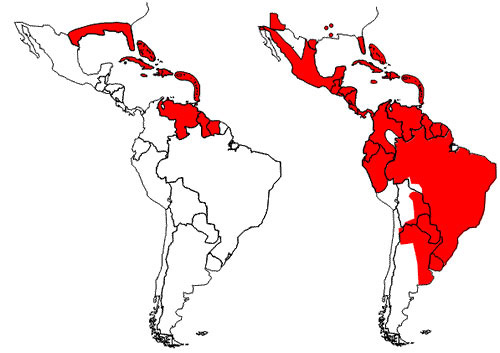
Reinfestation by the yellow fever mosquito, Aedes aegypti (Linnaeus), in the Americas, as of 2002. Left image shows reduction of range resulting from the eradication programs beginning in the mid-1990s. Right image shows re-infestation resulting from the end of the eradication programs. Illustration by PAHO/WHO 2002.
http://entnemdept.ufl.edu/creatures/aquatic/aedes_aegypti.htm
There are, of course, many other factors that have made possible this global epidemic such as increase in human urban population and greater mobility by many transport means of vectors and infected host from one continent to other. And there are many more conspiracy theories about its origin, but I am not going to mention examples or add links of the latter.
The epidemiology of Chikungunya fever (the way it is distributed, spread and is limited or reduced) depends greatly on the presence of its vector (female Aedes aegipty/albopictus), mosquitoes reservoirs and, obviously, infected host available to be bitten by the mosquito.

An adult Aedes can live from two weeks up to a month and during its entire life it can fly no more than 500 metres. Therefore, if there are no hosts 500 metres around your house, even if you are bitten by the mosquito it is very unlikely that you will get infected by the virus or if there are not reservoirs 500 metres from you it is difficult to think on a way someone could get the virus in their blood stream.
In the same way if you avoid being bitten using chemical or physical barriers or if there is an intervention on the vector's life cycle that could stop the reproductions of an important number of mosquitoes.
I am going to quote one meta-analysis that support the idea that mosquito nets impregnated with with a safe amount of pesticide can reduce malaria infections in 50% but there are other articles that do not give you the same level of confidence.
The effectiveness of insecticide-impregnated bed nets in reducing cases of malaria infection: a meta-analysis of published results.
There are companies that have being offering solutions to the problem of insect pests and this technology has been used to reduce the population of Dengue and Chikungunya vectors. The best known is SIT or the well-established radiation-based Sterile Insect Technique that makes male mosquitoes sterile. When these male Aedes are freed in the areas infested compete with the wild males and the female that mate with them will have offspring which will not reach adulthood.http://www.oxitec.com/news-and-views/topic-pages-safety-and-sustainability/ridl-sit-and-dengue-fever/
There are many strategies put in place since more than a decade already and at the moment I am writing this publication experimental vaccines are tested and probably billions of American dollars are spent preventing and treating Dengue and Chikungunya fever.
It is my view that affected countries' government, Non-governmental Organizations (NGO's) and communities have a lot more to do meanwhile definite treatment and vaccine available and affordable.
The first step should be the distribution of appropriated information in dense populated communities but in small groups at the time giving a real sense of responsibility over those who live next to you (200 - 500 metres around) and awareness of the risk of having neighbours infected by the virus and vector reservoirs.
There have been many projects, programmes, scientific proves and other iniciatives during the last few decades around the world to control the vector but they have not found consistency from governments and communities here you have two examples:
An American initiative with the support of US-Aid
http://www.ehproject.org/PDF/Strategic_papers/SR7-BestPractice.pdf
A Cuban initiative with little public resources
http://www.bmj.com/content/338/bmj.b1959
These two projects, a huge initiative and a small and low-cost research, were successful but did not continued in time. They are only two from thousands globally.
I would like to conclude this publication remarking that there are enough scientific prove to state that this epidemic is not the product of a conspiracy but lack of political and the general public will to control the vector and find a efficient and affordable treatment and vaccine. Just like in our personal lives, what our global village is suffering today is a consequence of what we have done and we have not done in the past (talking about decades or centuries).